Why timing matters in healthcare

Medicine has spent over a century perfecting what to measure and what to prescribe, yet it has paid little attention to the simpler question: when? Your biology is not the same at eight in the morning as it is at eight at night. Your blood pressure, cholesterol level, many hormones, immune responses, or the speed at which your liver breaks down a drug, all rise and fall in a predictable rhythm across the 24-hour day. This article makes the case that the answer to “Does timing matter in healthcare?” is an emphatic yes, and that taking biological time – namely circadian time - seriously may be one of the most powerful, and most overlooked, opportunities in modern medicine. The application of circadian biology to clinical considerations is the foundation of an emerging field called circadian medicine, which will properly encompass the new dimension of time. To understand why timing matters, we first need to understand the remarkable clocks ticking inside every one of us.
What are circadian rhythms, and how are they regulated?
A circadian rhythm, from the Latin circa diem, “about a day”, is any biological cycle that repeats roughly every 24 hours and, by definition, must keep running even when all external time cues and influences are removed [1]. A circadian rhythm must therefore be spontaneously generated by an internal oscillator, or ‘clock’.
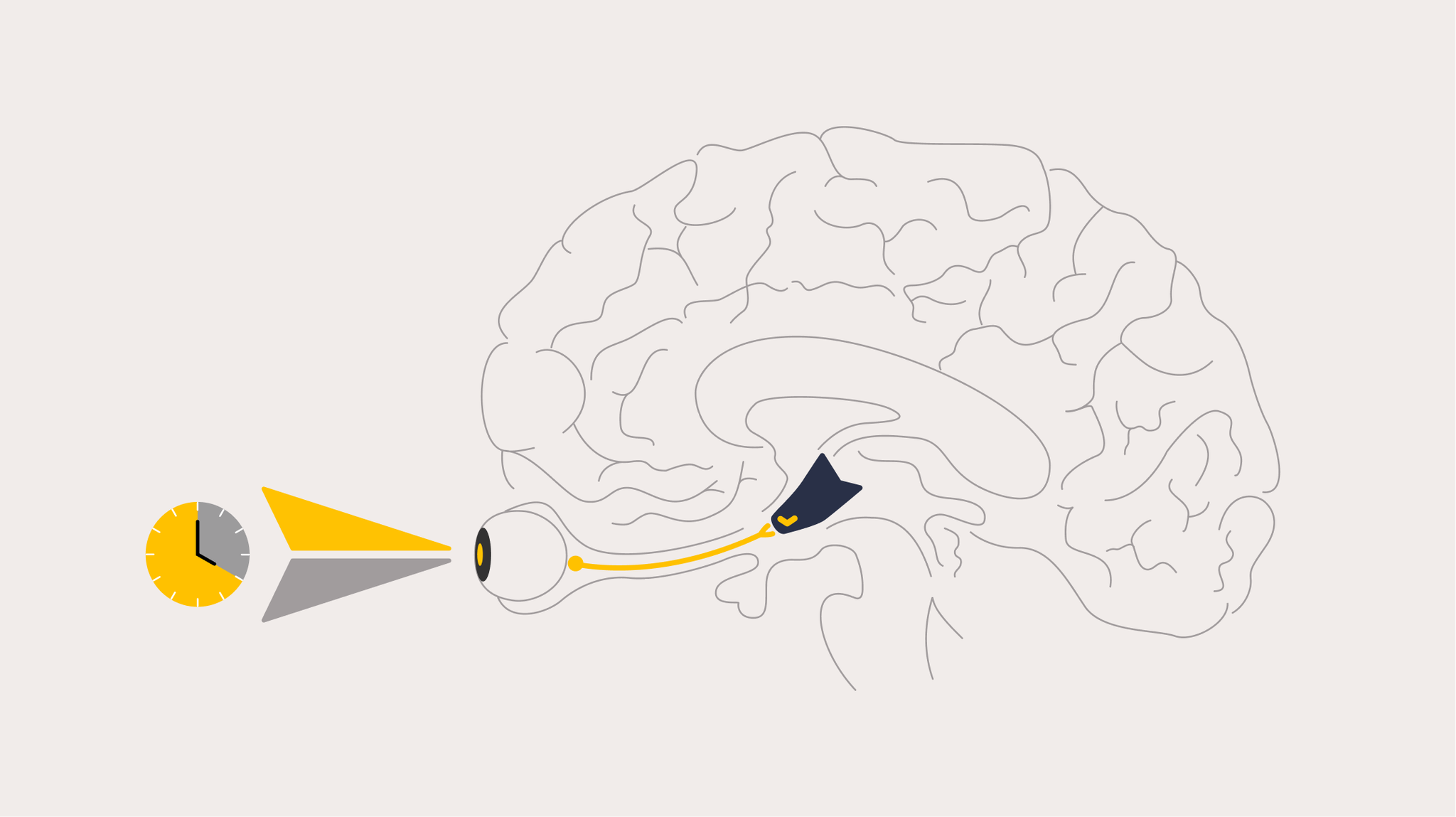
The main clock, or ‘conductor’ of this internal rhythmic orchestra is a tiny cluster of around 50,000 nerve cells deep in the brain called the suprachiasmatic nuclei, or SCN, sitting in the hypothalamus. The SCN is considered the central circadian pacemaker. Left entirely to its own devices, in constant dim light and no other time cues, the human clock does not run on exactly 24 hours – on average it runs slightly long, close to 24.2 hours, with a normal range across people from roughly 23.5 to 25.0 hours, with individual differences due to differences in a number of clock genes that generate these rhythms [2]. As the internal clock does not run at exactly 24 hours, it needs to be reset each day to the 24-hour day to remain appropriately synchronized to the environment, a process called entrainment.
The main environmental time cue that resets the clock is the daily light-dark cycle. Special light-detecting cells in the ganglion cell layer of the eye, separate from the rods and cones used for vision, contain a light-sensitive pigment called melanopsin that detect light and sends a signal directly to the SCN [3]. These cells are most sensitive to short-wavelength (blue) light, which is why the daily pattern of daylight exposure helps anchor the clock and why exposure to blue-light emitting screens in the evening can reset the clock to the wrong time, altering entrainment and misaligning the clock from behavior [4]. The central clock sends signals to other parts of the brain and body to control the timing of nearly all physiological processes including sleep, alertness, performance, many hormones, metabolism, immune responses and even reproductive function [5].
This regulation of circadian time is crucial to ensure physiology, metabolism and behavior all occur at the appropriate time relative to environmental time – external synchronization – and with each other – internal synchronization [5]. These are not random fluctuations to be averaged away – they are the carefully scheduled output of a clock that evolved to anticipate the predictable rhythm of day and night, allowing the organism to predict tomorrow and to therefore be awake at the right time to find food, find a mate, and avoid predators. When behavior occurs at the wrong circadian phase, for example when shift workers work, eat and sleep at the ‘wrong’ biological time – we pay a measurable price, including more accidents and injuries, reduced sleep and performance and impaired regulation of metabolic process, resulting in a higher risk of heart disease, obesity and diabetes, among many other negative effects [6].
App for shift workers
Timeshifter's shift work app is an entirely new way for shift workers to optimize their sleep, alertness, and quality of life. Import your work schedule to get highly personalized advice.
Learn more

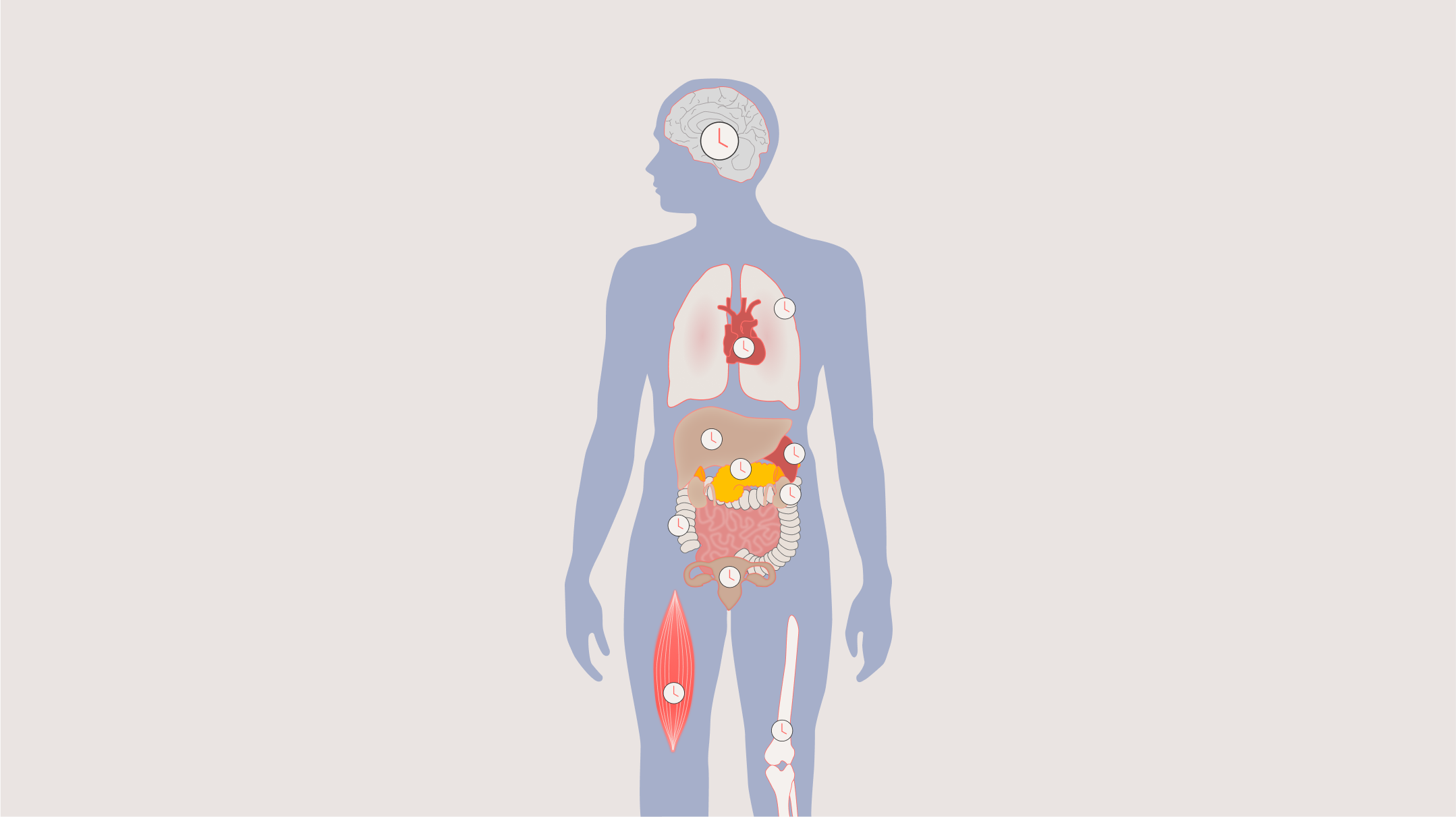
Clocks in every organ: Peripheral clocks
For a long time the SCN was thought to be the only clock. We now know that almost every tissue in the body, including the liver, heart, lungs, kidneys, pancreas, ovaries, skin and bladder, contains its own molecular clock, built from the same set of ‘clock genes switching each other on and off in a roughly 24-hour loop [7] Even though each peripheral clock can keep its own time, the SCN acts as the conductor that keeps these peripheral clocks playing in time with one another and then with the outside world [5]. When researchers mapped gene activity around the clock across a dozen organs, they found that nearly half of all protein-coding genes cycle with a 24-hour rhythm somewhere in the bod [9]. Your genome is, quite literally, a different place at different times of day.
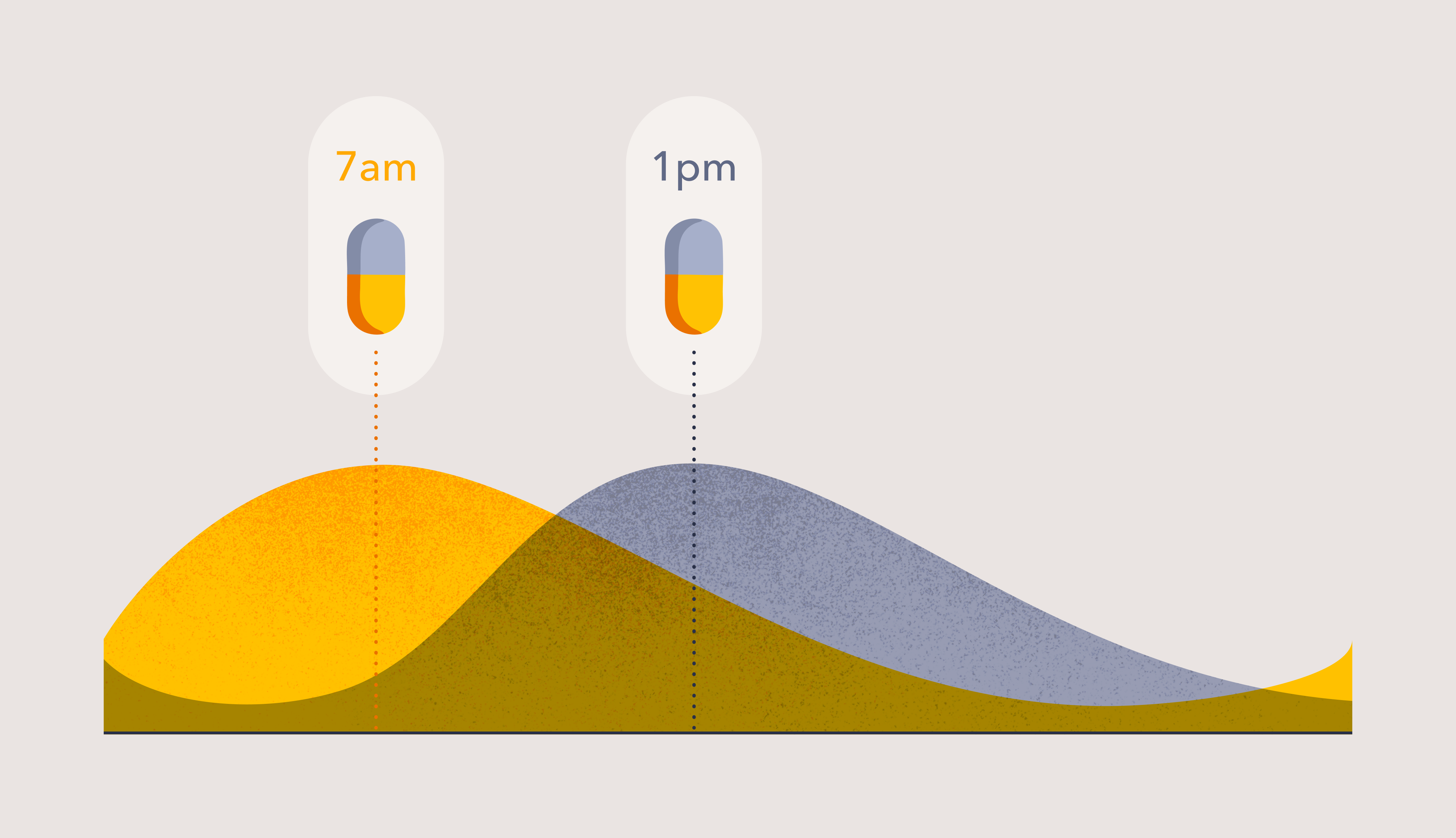
The liver clock deserves special attention, because the liver is the body’s chemical factory and the main site where medications are broken down. The genes that produce drug-metabolizing enzymes and transporters are themselves under circadian control, so the very machinery that absorbs, activates and clears a drug runs faster at some times than others [8]. The practical consequence is profound: the same pill, swallowed at the same dose, can reach a different concentration in your blood and act on a different level of its target depending on when you take it. Furthermore, the cellular receptors that detect and respond to these drugs also have their own circadian rhythms, meaning that even if the circulating dose is the same, the biological response can differ by circadian time. Thousands of approved drugs act on, or are processed by, proteins that follow a daily rhythm [8,9]. This is the biological foundation for everything that follows.
Chronodiagnostics: Reading a test result in the context of circadian time
If physiology changes across the day, then a single measurement, for example a blood test, a hormone level, a blood-pressure reading, is only part of the picture. A high cortisol reading in the morning may be normal but the same result in the afternoon may not [10]. Similarly, a high cholesterol reading in the afternoon is normal, but the same reading would be abnormal in the morning [11]. Interpreting tests in the context of the time at which is was taken is sometimes called chronodiagnostics, and it matters more than most clinicians realize.
The interpretation is even more complex than currently understood. The obvious workaround, to use sleep timing as a ‘proxy’, turns out to be surprisingly unreliable. The relationship between when you sleep and where your clock actually sits varies enormously from person to person. Clock time, currently used as the definition of time in clinical assessments, does not represent internal circadian time.
The period or cycle length of the circadian clock determines something called the ‘phase angle of entrainment’, that is how your individual circadian clock aligns with the daily light-dark cycle. Even when people have the same light-dark exposure or sleep-wake pattern, there are differences in the timing of the circadian clock based on how quickly the internal clock runs. Some people have an earlier circadian phase, and these people have a shorter circadian period (e.g., 23.8 h) whereas others have a later circadian phase, and have a longer period (e.g., 24.5 h) [2]. When studied under controlled laboratory conditions, there is a 5-6 hour range in circadian time even when people are exposed to the same light dark cycle [12, 13]. In the real-world, this range broadens to 8 hours in insomnia patients [14] and 9 hours in undergraduate students [15]. This means that measuring something at the same clock time in different people will represent a very different biological time in each of them; for example, an 8am blood test may be at the biological equivalent of 5am for some people, or 11am for others, requiring a different interpretation based on circadian time. As a rough rule of thumb (although this will change with age), morning chronotypes tend to have a shorter circadian period and evening types a longer one, and so an 8am blood test is actually occurring at a later circadian time for morning types (i.e., 11am) and an earlier circadian time for evening types (i.e., 5am).
There is a further complication, which requires a deep understanding of circadian biology to avoid making mistakes, and that is the issue of ‘masking’. Most rhythmic variables are, to some extent, affected directly by external factors which ‘mask’ the expression of the pure internal clock rhythm [10]. For example, core body temperature is directly increased by activity and decreased by sleep, and the observed rhythm can be perturbed to the extent that the timing of an unsupervised temperature rhythm can be out by as much as 12 hours compared to internal circadian time [16]. This makes temperature a unreliable marker of circadian time in the real world. Other factors affect different rhythms – light suppresses melatonin directly and stress elevates cortisol, as two examples. The clinical warning is clear: a rhythmic test measured in ordinary daily life is a blend of the true circadian clock time plus substantial behavioral noise, and confusing the two is a recipe for false positive and false negative interpretations. This is why interpreting a test, or timing a drug, by clock time alone is a blunt instrument. To know circadian time, you have to measure it.
Measuring circadian time
There are ways to address these concerns, however. To observe the clock’s genuine output, scientists use a laboratory method called the constant routine, in which a volunteer stays awake in constant dim light, semi-reclined, taking identical small snacks every hour for at least 24 hours, so that the masking effects of behavior are removed or spread evenly across the day [17]. Only then does the real endogenous rhythm reveal itself. Typically, the same measurements are also taken the day before, during a ‘normal’ laboratory day with a standard sleep-wake and dark-light cycle, three standard meals and fewer postural restrictions. By comparing the baseline and constant routine data, scientists can observe how well the baseline timing matches the internal circadian time and therefore ascertain the suitability of using that measure in the real world [10, 11]. Using these methods, it is possible to create a handbook of clinical norms by circadian time (not just one time) and how the result may vary under real world conditions.
In practice, this means that clinical tests need to be performed alongside a measurement or reliable model prediction of circadian time in order to interpret the results properly. There are a number of ways to do that, and new methods are currently in development. The most common current methods involve measuring either the onset of melatonin release in saliva, while exposed to dim light over 6-8 hours in the evening (called the Dim Light Melatonin Onset, DLMO) [18], or the entire rhythm of the melatonin metabolite 6-sulfatoxymelatonin or cortisol by collecting serial urine samples over at least 24 hours, which has the advantage of capturing the whole rhythm and is harder to ‘miss’ [19, 20]. These are well-established techniques, used in thousands of studies, where the interpretation and risks of masking are understood in detail.
More recently, there have been a number of efforts to measure circadian time from a single blood, saliva, urine or even breath sample taken at any time of day. These approaches take advantage of new technology allowing measurement of potentially thousands of different molecular features in the same sample and using machine learning to infer the clock’s position. These ‘omics’-based methods can measure metabolites (metabolomics), transcription factors (transcriptomics), lipids (lipidomics) or proteins (proteomics). While a number of studies have shown promise in predicting circadian time using these methods under controlled laboratory conditions [21-24], they are yet to be validated in real world settings where the risks associated with masking are not yet known. Developments in continuous monitoring devices, as currently widely used to measure glucose continuously to help manage diabetes, may also allow measurement of reliable circadian rhythms over 24 hours or more outside of the laboratory. The goal is to produce a rapid, reliable, inexpensive measurement of circadian time at the point-of-care, or even at home, and will become as quick and easy as measuring blood pressure or glucose, but with more universal applicability. It would let us interpret blood tests against norms set for your circadian time and it would tell us the right moment to administer a particular drug. That single capability – measuring an individual’s clock cheaply and instantly – is the foundation on which truly personalized circadian medicine will be built.
Application of circadian medicine
Circadian rhythm sleep-wake disorders
Nowhere is the need to measure circadian time clearer than in the diagnosis and treatment of circadian rhythm sleep-wake disorders – conditions such as delayed and advanced sleep-wake phase disorder, non-24-hour sleep-wake disorder (common in people who are totally blind), and the disruption of shift work and jet lag. In all of these, the core problem is that sleep is being attempted at the wrong biological time. You simply cannot diagnose them properly, or time their treatment with light or melatonin correctly, without knowing or modeling where the patient’s clock actually is. Given that light and melatonin can reset the clock either earlier or later depending in the circadian time of exposure, treating these disorders using clock time, or a one-size-fits-all approach, can push the clock the wrong way and make matters worse [25, 26].
Jet lag is history.
Timeshifter's jet lag app is the most downloaded and highest-rated jet lag app in the world. Get personalized jet lag plans based on your sleep pattern, chronotype, itinerary, and personal preferences.
Learn more

Chronotherapeutics: Does the timing of treatment change the outcome?
If diagnosis depends on circadian time, so does treatment. Chronotherapeutics is the study of how the timing of a drug, a procedure or an operation changes how well it works and how much harm it causes. The idea is not new – pioneers such as William Hrushesky showed decades ago that appropriately timing cancer chemotherapy could reduce its toxicity [27], and chronotherapy for blood pressure was proposed over 15 years ago [28] – but it has gained fresh momentum as the molecular biology has caught up. A systematic survey of more than a hundred clinical trials spanning fifty years found that around three-quarters reported that the efficacy or toxicity of treatment depended on the time of day it was given, across conditions as common and consequential as high blood pressure, asthma, arthritis and cancer [9].
The examples span much of everyday medicine. To treat high cholesterol levels, the short-acting statin simvastatin works better taken in the evening [29]. In asthma, where airways narrow most overnight, evening-weighted bronchodilator therapy better matches the drug to the night-time worsening of symptoms [30]. In rheumatoid arthritis, a modified-release night-time prednisone designed to reduce morning stiffness worked better than standard daytime dosing [31]. Even surgery can show the effect. In one study, patients undergoing heart-valve surgery in the afternoon suffered less heart-muscle injury than those operated on in the morning, a difference traced to a clock gene and reproducible in the laboratory [32].
Vaccines are a particularly clean illustration, because the immune system is so strongly rhythmic. A cluster-randomised trial found that older adults given a morning influenza vaccine produced more antibodies than those vaccinated in the afternoon [33]. The principle extended to the pandemic: in an observational study of around 1.5 million people, the time of day of COVID-19 vaccination was associated with differences in protection [34]. Reviews and meta-analyses now broadly support a morning advantage for several vaccines, while sensibly cautioning that the picture is not uniform and that the optimal time may itself depend on an individual’s circadian phase rather than clock time [35, 36].
Cancer deserves only a brief mention here, because it merits an article of its own. Building on Hrushesky’s early work, Francis Lévi and colleagues showed in randomized trials that delivering colorectal-cancer chemotherapy on a ‘circadian’ schedule could change both tolerability and effect [37]. More recently, the timing of immunotherapy has produced some of the most striking signals in all of oncology: in advanced melanoma, patients who received most of their immune-checkpoint infusions earlier in the day lived substantially longer than those treated later, a pattern since echoed by meta-analysis across several cancers and reinforced by recent studies in lung cancer [38-40]. These are observational findings that demand confirmation in proper randomized trials – but the size of the apparent effect is hard to ignore.
While these findings are encouraging, much more work remains to be done. None of the studies published to date have timed drugs according to individual circadian time – they have only compared different times of day which, as explained above, does not represent circadian time. Even when comparing morning versus evening dosing, there may be still be an overlap in the circadian time of administration between the groups given the wide inter-individual variation in internal time. As previously explained, an 8am clock time administration could represent anywhere from 4am to 12pm in biological time, and a 4pm dose could represent anywhere from 12pm-8pm in different individuals. This may explain why some studies do not find time of day differences in outcomes [41]. Only when drugs or procedures are timed relative to individual circadian time can the full extent of the clock’s impact be observed, and the genuinely important opportunities identified.
Building circadian time into clinical trials
It is now clear that circadian time should be included as an important variable in all stages of clinical trials. Most trials prescribe drugs at the same clock time for everyone, or use vague instructions like ‘morning’ or ‘bedtime’. Given that internal clocks vary by up to 8 hours across a population, a trial that dosed everyone at ‘8am’ actually dosed them across a wide and unrecorded spread of biological times. If timing changes a drug’s effect, that hidden variation adds scatter that can blur a genuine signal into apparent failure.
There is a pragmatic, low-cost way forward. The first step is simply to add circadian time alongside existing trials, recording each participant’s internal time without otherwise changing the protocol. Until the single-sample circadian methods are validated and available, circadian phase can be measured from saliva or urine as outlined above. These are non-invasive, reliable and relatively inexpensive additions compared to the cost of a clinical trial, and might provide invaluable additional knowledge to the drug approval process.
Once circadian time is added, it is relatively straightforward to analyze the results with respect to the circadian time at which the drug was given and, if there is a positive signal, the second step would be a prospective trial that randomizes participants by circadian tim, dosing relative to each person’s internal clock, and compares it against current standard practice, which usually means a fixed clock time, mealtime or bedtime. This staged approach lets the data, rather than guesswork, decide when circadian dosing is worth the effort. Cardiovascular medicine is already moving in this direction, with new chronotherapy trial frameworks and randomized statin-timing studies now being launched explicitly to settle these questions [42].
The potential payoff is enormous, and not only for patients. Bringing a new drug to market costs vast sums, and the great majority of compounds that enter clinical testing never reach patients – many failing not because the molecule is useless but because a real effect was too small or too variable to prove. The most commonly prescribed drugs do not help the people who take them equally, and the usual response is a call for better genetic precision [43]; yet circadian effect sizes can be just as large as genetic ones, and basing drug use on individual genetic testing would be much more complex to operationalize. If even a small fraction of trials that previously failed would have succeeded had circadian time been taken into account, the consequences would be measured in billions of dollars saved and, far more importantly, in effective treatments rescued from the scrapheap and delivered to people who need them. Timing is not a marginal tweak to the drug-development pipeline; it could be a lever on its overall success rate.
While determining individual drug timing would be quite straightforward once the data are available, it has sometimes been claimed that personalizing the time of procedures by circadian time would add an unmanageable burden to clinics. In this case, the answer would be to shift the clock to match the appointment time, rather than alter the clinical schedule to match the patient. Shifting the clock to a new time, essentially a new ‘time zone’, is the basis of Timeshifter’s Jet Lag and Shift Work apps, but would be applied in the context of clinical appointments. For example, a patient might have a 10am vaccine appointment but the best circadian time to have the vaccine is the biological equivalent of 8am. The patient’s clock can therefore be shifted later by 2 hours using the same approach as for jet lag and shift work, so that the appointment time now coincides with the correct circadian time, and then shifted back after.
The bottom line: A clinic that finally tells the time
So, does timing matter in healthcare? The biology leaves little room for doubt. A clock in the brain, backed by clocks in every organ, schedules our hormones, metabolism, immune defenses, bone turnover and DNA repair across the day, and shapes how we process the drugs we are given. The clinical implications follow directly, and they can be distilled into four ideas to consider.
First, we can already model circadian phase and measure it with traditional methods, and we continue to seek faster, better ways to measure and predict day-to-day changes in the clock so that advice can be tailored to your internal time rather than social time. Second, a quick, accurate, inexpensive point-of-care or home-based measure of circadian phase would revolutionize medicine in ways we cannot yet fully predict, doing for circadian time what the thermometer did for temperature. Third, individual circadian-phase measurements will enable more accurate diagnoses, with clinical norms based on circadian phase and personalized to your own clock, so that a test result is finally read in the context of the biological time it was taken. And fourth, because so many medications show a daily rhythm in how well they work and how much harm they cause, circadian-phase measurement will allow drugs, procedures and surgery to be timed more effectively – personalized, once again, to your circadian clock.
Modern medicine has become extraordinarily good at deciding what to do for a patient. The next frontier is learning when to do it. As the tools to measure and model circadian time become better and more accessible, circadian medicine will move from the laboratory to the bedside – and the clinic of the future will, at last, take time properly into account.